Shoulder Surgery: Diagnosis, Treatment Options & Recovery
We deliver diagnosis-first care, favouring conservative management where safe and precise shoulder surgery when necessary. Our integrated surgeons–physiotherapists team focuses on restoring comfort, strength, and confidence for overhead activity, work, and sport.
Common Conditions
Shoulder Arthroscopy
Key hole surgery uses a camera called an arthroscope to repair the tissues inside your shoulder joint.
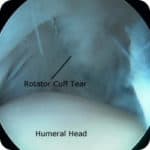
Rotator Cuff Tear
A rotator cuff tear is a common tear of the shoulder that causes pain and difficulty moving the arm
Who We Help
We care for active adults, workers, and athletes with pain on reaching or lifting, night pain, weakness, clicking, and instability. Whether symptoms followed an injury or developed gradually, we provide a clear plan from first assessment through to full recovery.
Our Treatment Philosophy
- Accurate diagnosis through targeted history, examination, and appropriate imaging.
- Conservative-first: education, load modification, and criteria-based rehabilitation.
- Right operation, right time: arthroscopic repair/reconstruction for mechanical problems; anatomic or reverse shoulder replacement for advanced arthritis or cuff-deficient shoulders.
- Integrated rehab with objective milestones for a safe, confident return to activity and sport.
Shoulder Conditions We Treat
- Rotator Cuff Tear
— pain with overhead use, weakness, night pain - Subacromial Impingement / Bursitis
— painful arc, discomfort with reaching - Shoulder Instability & Dislocation
— apprehension in abduction–external rotation - SLAP Tear & Biceps Pathology
— deep click, overhead/throwing athletes - Frozen Shoulder (Adhesive Capsulitis)
— stiffness with global motion loss - AC Joint Arthritis
— top-of-shoulder pain, cross-body pain - Calcific Tendinitis
— severe night pain, acute flares - Glenohumeral Osteoarthritis
— grinding, stiffness, loss of rotation
Shoulder Surgery & Procedures
Shoulder Arthroscopy (Keyhole Surgery)
Minimally invasive procedures to restore tendon function, stabilise the shoulder, and settle subacromial pain. Learn more: Shoulder Arthroscopy.
- Rotator cuff repair (single/double-row, augmentation in selected cases).
- Subacromial bursectomy and decompression when indicated.
- Bankart repair for soft-tissue instability; remplissage in engaging Hill–Sachs lesions.
- Biceps tenodesis/tenotomy for symptomatic SLAP/biceps disease.
- AC joint excision for refractory AC joint arthritis.
Stability Surgery
For recurrent dislocations or significant bone loss. Learn more: Bankart Repair and Latarjet Procedure.
- Arthroscopic Bankart with capsular plication for soft-tissue instability.
- Latarjet coracoid transfer for glenoid bone loss or high-risk athletes.
Shoulder Replacement
Reliable pain relief and function for advanced arthritis or irreparable cuff deficiency. Learn more: Anatomic Replacement and Reverse Replacement.
- Anatomic total shoulder for intact rotator cuff and concentric wear.
- Reverse total shoulder for cuff tear arthropathy, complex fractures, or revisions.
- Personalised implant selection and enhanced recovery protocols.
Non-Operative Care
Many shoulders improve without surgery. We tailor education, load modification, and exercise therapy with our physiotherapy team.
- Rotator cuff & scapular control: strength and coordination for overhead tasks.
- Mobility for capsule and soft tissues within symptom-guided ranges.
- Hydrodilatation or corticosteroid injection for frozen shoulder/subacromial bursitis when indicated.
- Gradual return-to-throw/work programs with criteria-based progressions.
Diagnosis & Imaging
We combine targeted examination and imaging to confirm diagnosis and plan care:
- Clinical tests for cuff strength, impingement signs, biceps/labrum, and instability.
- X-rays for acromial shape, AC joint, glenohumeral alignment, and arthritis.
- Ultrasound for dynamic cuff/bursal assessment; MRI/CT to define tendon quality, labrum, bone loss.
Recovery & Timelines
After Arthroscopy (Bursectomy/Decompression)
- Days 1–7: pain control, early range, sling for comfort only.
- Weeks 2–6: progressive strength and function; desk work often 1–2 weeks.
- Weeks 6–12: return to heavier tasks and sport practice as criteria are met.
After Rotator Cuff Repair
- Weeks 0–4: sling protection, passive/assisted range per protocol.
- Weeks 6–12: active range and strengthening; light duties as guided.
- Months 4–6+: work/sport progressions; overhead/throwing later with objective testing.
After Instability Surgery
- Weeks 0–4: sling, protected range; avoid abduction–external rotation early.
- Weeks 6–12: strength and neuromuscular control; running/non-contact skills as allowed.
- Months 4–6+: contact sport after criteria-based testing.
After Shoulder Replacement
- Hospital & early phase: early hand/elbow use; guided shoulder range.
- Weeks 2–6: functional independence, daily activities.
- Weeks 6–12: progressive strength; driving/desk work as advised.
- Beyond 3 months: low-impact activities (swimming, cycling, golf) per guidance.
Ready to Take the Next Step?
If shoulder pain or instability is limiting work, sleep, or sport, we’ll help you move forward with a clear diagnosis and plan.
Shoulder Surgery — FAQs
Do all shoulder problems need surgery?
No. Many conditions respond to education, load modification, injections when indicated, and structured physiotherapy. Surgery is considered when pain, weakness, or instability persists or when there is a repairable mechanical issue.
Rotator cuff tear: repair or physiotherapy?
Both are valid depending on age, activity, tear size/quality, and goals. We favour repair for acute traumatic tears and younger active patients; degenerative tears may start with a structured rehab trial.
Bankart vs Latarjet — which is right for me?
Bankart repair suits soft-tissue instability without significant bone loss. Latarjet is considered for glenoid bone loss, engaging Hill–Sachs lesions, contact athletes, or revision instability.
Anatomic vs Reverse shoulder replacement?
Anatomic is used when the rotator cuff is intact. Reverse is preferred for cuff-deficient shoulders, complex fractures, or revisions. We match implant choice to anatomy and goals.
When can I drive and return to sport?
Driving typically resumes once you are off strong analgesia and can safely control the vehicle, often around 2–6 weeks depending on procedure. Return to sport is criteria-based and varies from weeks (bursectomy) to months (cuff repair, stabilisation, replacement).
What are the risks?
All surgery carries risks: infection, bleeding, clots (rare), stiffness, nerve irritation, re-tear or recurrence, and anaesthetic risks. We discuss personalised risk and prevention strategies at consultation.